When you’re struggling with severe obesity, losing weight isn’t just about willpower. It’s about biology. Your body fights to keep the weight on, no matter how hard you try. That’s where bariatric surgery comes in. Two procedures dominate the field today: gastric bypass and sleeve gastrectomy. Both help you lose weight. But they work in very different ways. And the choice between them can change your life - for better or worse.
How These Surgeries Actually Work
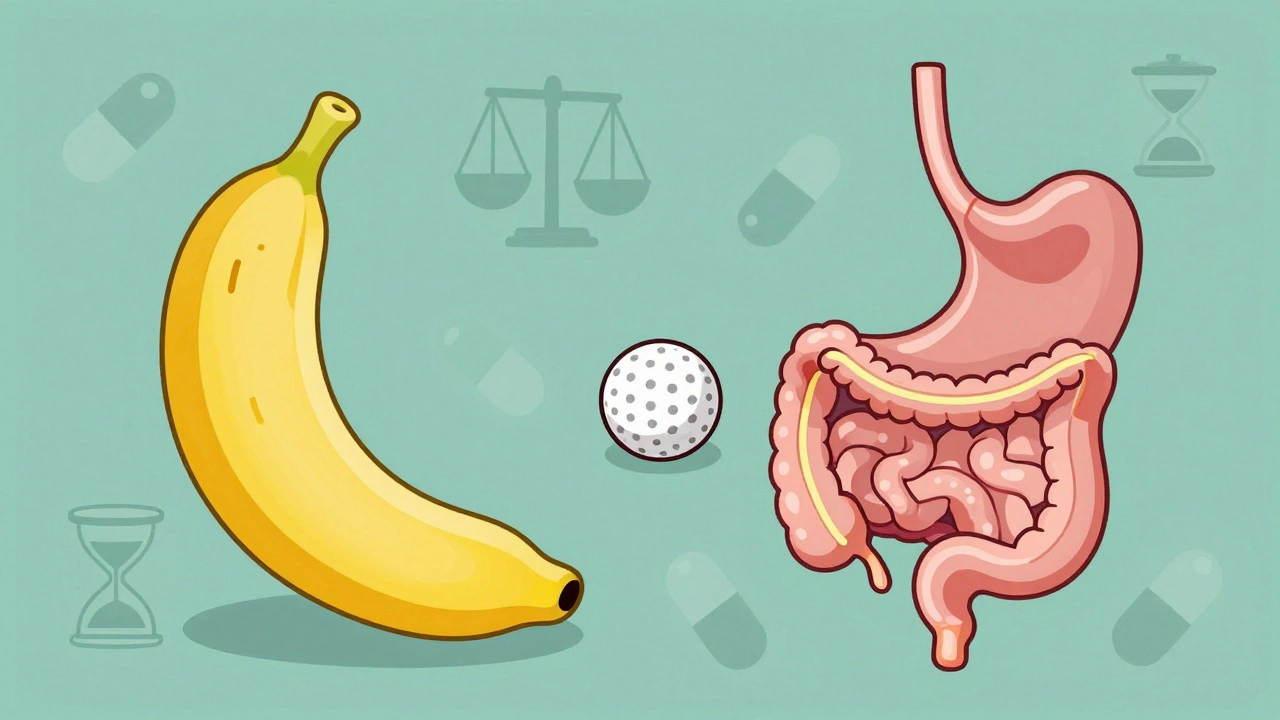
Gastric bypass, also called Roux-en-Y, doesn’t just shrink your stomach. It reroutes your digestive system. Surgeons create a small pouch - about the size of a golf ball - from the top of your stomach. Then they connect it directly to the middle part of your small intestine, skipping most of the stomach and the first section of the intestine. That means food doesn’t get digested the same way. You absorb fewer calories. You also get changes in gut hormones that make you feel full faster and less hungry.
Sleeve gastrectomy is simpler. About 80% of your stomach is removed. What’s left is a narrow tube, shaped like a banana, holding just 2 to 5 ounces. That’s it. No rerouting. No bypassing. Just a smaller stomach that fills up quicker. You eat less because you physically can’t fit much in.
The surgery time reflects the difference. Sleeve gastrectomy takes about 47 minutes on average. Gastric bypass? Around 68 minutes. That’s not just a few extra minutes - it’s a more complex operation with more steps, more risks, and more things that can go wrong.
Weight Loss: Who Loses More?
If your main goal is to lose the most weight possible, gastric bypass usually wins. Studies show that five years after surgery, people who had gastric bypass lost about 57% of their excess weight. Sleeve gastrectomy patients lost around 49%. That’s a noticeable difference.
UPMC data shows gastric bypass patients often lose 60-80% of excess weight within 12 to 18 months. Sleeve patients lose 60-70% over the same time, but it tends to happen more slowly. That doesn’t mean sleeve doesn’t work - it does. But if you’re looking for the biggest drop, bypass has the edge.
Still, weight loss isn’t just about numbers. It’s about how you feel. Some people on the sleeve report feeling hungrier long-term. Others on bypass say they get sudden, unpleasant side effects - like dumping syndrome - after eating sugar or fatty foods. That’s when food moves too fast into the intestine, causing nausea, sweating, dizziness, and cramps. About half to 70% of bypass patients experience it at least once.
Health Improvements: Diabetes, Blood Pressure, and More
Both surgeries improve or even reverse serious health problems. High blood pressure, type 2 diabetes, sleep apnea, and joint pain often get better - sometimes within days.
But here’s the catch: gastric bypass has a stronger effect on metabolic conditions. A 2024 JAMA Network Open study found hypertension improved more often in bypass patients. Dr. Amir Ghaferi from Michigan Bariatric Surgery Collaborative says the malabsorptive part of bypass helps resolve diabetes better than sleeve in many cases. That’s because bypass changes gut hormones more dramatically, which directly affects how your body handles sugar.
That doesn’t mean sleeve doesn’t help. Many people with type 2 diabetes see their blood sugar normalize after sleeve surgery. But if you have severe diabetes, bypass might give you a better shot at getting off insulin.
Risks and Complications: What Can Go Wrong?
Both surgeries are safe - but not risk-free. The big difference is in long-term safety.
A 2022 study of over 95,000 Medicare patients found sleeve gastrectomy had a lower 5-year death rate: 4.27% compared to 5.67% for gastric bypass. That’s a 32.8% lower relative risk of dying. That’s huge.
Sleeve patients also have fewer overall complications - infections, leaks, blood clots. But here’s the twist: they’re more likely to need a second surgery. The same study showed a 3.2 percentage point higher revision rate for sleeve patients over five years. Why? Because the stomach can stretch over time. Some people start gaining weight back. Others develop severe reflux.
Gastric bypass has its own risks. Malabsorption means you’re more likely to get deficiencies in iron, vitamin B12, calcium, and folate. That’s not just a minor inconvenience - it can lead to anemia, nerve damage, or osteoporosis. That’s why bypass patients need blood tests every six months, not once a year. And they need to take supplements for life.
Another risk unique to bypass is internal hernias - when loops of intestine get trapped in gaps created during surgery. In the past, this happened in 2-5% of cases. Now, with modern techniques like closing the Petersen space, that rate is below 1%.
Recovery and Lifestyle: What’s Easier?
Recovery time is similar - about 2 to 4 weeks. But what you can eat after surgery? That’s where things split.
Sleeve patients usually have fewer dietary restrictions early on. You can eat more types of food, and you’re less likely to get dumping syndrome. That’s why many people say recovery feels easier.
But bypass patients have to be stricter. They can’t eat sugary or fatty foods without paying the price. They also need to chew food longer, eat smaller bites, and avoid drinking with meals. If they don’t, they’ll feel awful.
On the flip side, bypass patients often report feeling full faster and staying full longer. Some say they don’t crave food the way they used to. That’s the hormone effect at work.
Cost and Insurance: What’s Affordable?
Sleeve gastrectomy is cheaper. On average, it costs about 25% less than gastric bypass. In Q3 2024, out-of-pocket costs were $14,500 for sleeve versus $19,300 for bypass - assuming insurance covers 80%.
Insurance rules are strict. Most require a BMI of 40 or higher, or 35 with conditions like diabetes or high blood pressure. But some insurers, like UnitedHealthcare, now require a BMI of 45 as of January 2024. You’ll also need to prove you’ve tried other weight loss methods for at least six months. That means doctor visits, counseling, and sometimes a supervised diet program.
Why Is Sleeve Gastrectomy So Much More Popular?
In 2022, 63.2% of all bariatric surgeries in the U.S. were sleeve gastrectomy. Only 27.4% were gastric bypass. That’s a huge shift. In 2010, sleeve made up less than 10% of procedures.
Why? Because it’s simpler, safer, and cheaper. Surgeons prefer it. Patients prefer it. And the data backs it up: lower death rates, fewer complications, shorter surgery time.
But here’s what most people don’t say: sleeve gastrectomy’s popularity doesn’t mean it’s better for everyone. It just means it’s easier to sell. And for many patients, that’s fine. But if you have severe diabetes, or you need the most weight loss possible, bypass might still be the right choice - even with the extra risks.
What About Future Options?
Surgeons are already working on hybrid procedures. Some are testing a “mini-bypass” - a smaller version of gastric bypass with fewer complications. Others are combining sleeve with a partial bypass to get the benefits of both. Clinical trials are underway at places like Mayo Clinic and Massachusetts General Hospital.
There’s also growing interest in endoscopic revisions. If you had a sleeve and started gaining weight back, you might not need another major surgery. New techniques can tighten the sleeve from the inside using a scope. That’s still experimental, but it’s promising.
Real People, Real Choices
On Reddit’s r/bariatrics, one patient wrote: “I had the sleeve. I lost 120 pounds. But I’m hungry all the time now. I thought it would be easier. It’s not.”
Another said: “Bypass was brutal. Dumping syndrome ruined my favorite foods. But I haven’t had a craving in five years. I’m not going back.”
There’s no one-size-fits-all answer. Your choice depends on your health, your goals, and your willingness to manage lifelong changes.
If you want the biggest weight loss and have diabetes, bypass might be worth the extra risk. If you want the safest, simplest path and are okay with slower results, sleeve is the way to go.
Both surgeries can give you your life back. But only if you choose the one that fits your body - not just your hopes.
Which surgery leads to more weight loss: gastric bypass or sleeve gastrectomy?
Gastric bypass typically leads to more weight loss. Five years after surgery, patients lose about 57% of their excess weight on average, compared to 49% with sleeve gastrectomy. Gastric bypass patients often lose 60-80% of excess weight within 12 to 18 months, while sleeve patients lose 60-70% over the same period, but at a slower pace.
Is sleeve gastrectomy safer than gastric bypass?
Yes, sleeve gastrectomy is generally safer. A 2022 study of over 95,000 patients found a 32.8% lower risk of death at five years compared to gastric bypass. Sleeve patients also have fewer complications like infections and nutritional deficiencies. However, they are more likely to need a second surgery later due to stomach stretching or worsening reflux.
Do I have to take vitamins for life after bariatric surgery?
Yes - but more so after gastric bypass. Because bypass changes how your body absorbs nutrients, you’ll need lifelong supplements for iron, vitamin B12, calcium, and folate. Blood tests every six months are recommended. Sleeve patients also need supplements, but less frequently - usually once a year - because the stomach still absorbs nutrients normally, just in smaller amounts.
Can I eat normally after sleeve gastrectomy?
You can eat more types of food after sleeve gastrectomy than after gastric bypass. But you’ll still need to eat smaller portions, chew slowly, and avoid overeating. Unlike bypass, you won’t get dumping syndrome from sugar or fat. However, some patients develop chronic reflux or feel hungry more often long-term.
Why is gastric bypass becoming less common?
Gastric bypass is becoming less common because sleeve gastrectomy is simpler, faster, cheaper, and has fewer immediate complications. In 2022, 63.2% of bariatric surgeries in the U.S. were sleeve procedures, up from under 10% in 2010. Surgeons and patients both prefer the sleeve because it offers strong weight loss with lower risk - even if bypass leads to slightly better long-term results for some.
What’s the recovery time for each surgery?
Recovery time is similar for both - about 2 to 4 weeks. Most patients go home after one day in the hospital. Sleeve patients often feel better faster because the surgery is less invasive. But both require strict dietary changes, and you’ll need to avoid heavy lifting and strenuous activity for at least six weeks.
Does insurance cover both surgeries?
Yes, most insurance plans cover both gastric bypass and sleeve gastrectomy if you meet the criteria: a BMI of 40 or higher, or a BMI of 35 with obesity-related conditions like diabetes or high blood pressure. Some insurers, like UnitedHealthcare, now require a BMI of 45. You’ll also need proof of prior weight loss attempts, psychological evaluation, and medical clearance.
Can I regain weight after bariatric surgery?
Yes, weight regain is possible with either surgery. About 15% of sleeve patients need some kind of intervention within five years, often due to stomach stretching or poor eating habits. Gastric bypass patients are less likely to regain weight, but it can still happen if they return to old eating patterns. Long-term success depends on lifestyle changes - not just the surgery.










Write a comment